
- Medi-Cal is a public health insurance program for low-income Californians.
Medi-Cal—California’s Medicaid program—is a state-federal program that offers free or low-cost health coverage to Californians with low family incomes. Prior to the Affordable Care Act (ACA), Medi-Cal served low-income families and children, the elderly, and people with disabilities. Under the ACA, California lawmakers expanded the program to include low-income adults without children or a qualifying disability starting in 2014. Total program costs are slated to be $98.5 billion in fiscal year 2018–19, with the federal government providing $62.7 billion, the state General Fund $20.7 billion, and other state sources—including funds generated by provider fees and transfers from local governments—another $15.1 billion. - Medi-Cal eligibility is determined by a combination of income and other factors.
To qualify for comprehensive Medi-Cal, most adults must have an annual income below about $17,250 for a single adult (138% of the federal poverty level or FPL) and satisfactory immigration status. Pregnant and postpartum women are eligible with incomes up to about $68,700 for a family of three (322% FPL), though women with incomes just under this threshold must make financial contributions. Children under age 19 are eligible if their family incomes are below about $56,750 for a family of three (266% FPL), regardless of immigration status. A more limited version of Medi-Cal covers undocumented adults in certain situations, such as medical emergency or pregnancy. - Medi-Cal provides 12 million Californians with comprehensive health insurance.
Enrollment in comprehensive Medi-Cal has increased rapidly in recent years, growing from about 8 million at the end of 2013 to more than 12 million (31% of the state) in August 2018. The limited version of Medi-Cal covers about 900,000 low-income undocumented adults, an additional 2% of the state’s population. In some counties, about half of residents are covered by either comprehensive or limited Medi-Cal.
About half of residents in some counties are enrolled in Medi-Cal
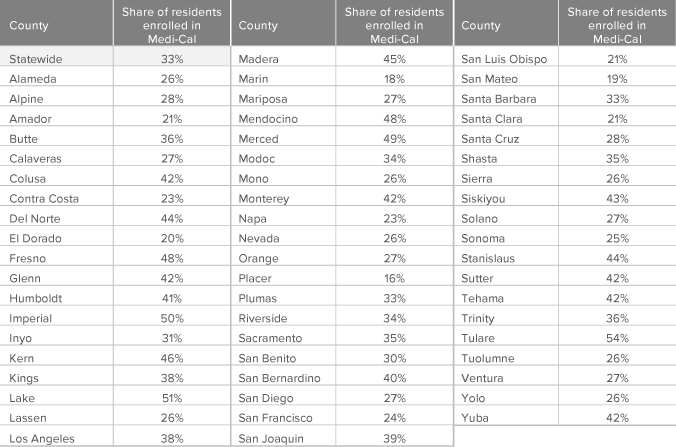
SOURCES: California Department of Health Care Services, Research and Analytic Studies Division, Medi-Cal Certified Eligibles County Pivot through August 2018 and California Department of Finance, Population Estimates for July 1, 2018.
NOTES: Numerator is total certified eligible enrolled in full-scope and limited-scope Medi-Cal. Denominator is total county population.
NOTES: Numerator is total certified eligible enrolled in full-scope and limited-scope Medi-Cal. Denominator is total county population.
- Families make up half of the Medi-Cal caseload but have lower costs.
Children and parents are the largest group of Medi-Cal enrollees, accounting for nearly half of the total caseload. Adults under 65 who gained eligibility under the ACA are the second-largest group (26% of enrollees), followed by seniors and people with disabilities (15%). The remainder of the caseload includes undocumented adults and other groups, such as those in foster care and long-term care. The caseload mix is a main driver of costs. The most recent data for California from 2014 indicate annual average costs per enrollee were lowest for children ($2,836) and adults under 65 ($3,913)—but significantly higher for seniors ($12,268) and individuals with disabilities ($20,222).
More than a quarter of Medi-Cal enrollees are adults who gained coverage under the ACA
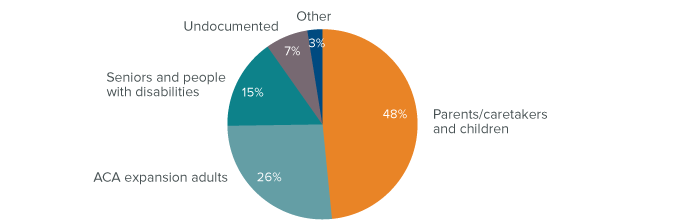
SOURCE: California Department of Health Care Services, Medi-Cal Monthly Enrollment Fast Facts, August 2018.
NOTES: Children and pregnant women receiving Medi-Cal benefits under eligibility categories associated with the Children’s Health Insurance Program (CHIP) are included in the share of parents and children. The ‘Other’ category comprises people in the following eligibility categories: adoption/foster care, individuals residing in long-term care facilities, and other unspecified groups.
NOTES: Children and pregnant women receiving Medi-Cal benefits under eligibility categories associated with the Children’s Health Insurance Program (CHIP) are included in the share of parents and children. The ‘Other’ category comprises people in the following eligibility categories: adoption/foster care, individuals residing in long-term care facilities, and other unspecified groups.
- Medicaid expansion is linked to improved outcomes.
Beyond substantially increasing insurance coverage, a growing body of evidence has linked Medicaid expansion under the ACA to improved outcomes across a number of domains. Individuals in states that expanded Medicaid experienced increased access to care, greater use of prescription drugs and preventive care, and improved financial well-being, including fewer bankruptcies, better credit scores, and reduced debt relative to those in states that chose not to expand. Medicaid expansion is also associated with improved financial performance at hospitals and a lower likelihood of hospital closures, especially in rural areas. - California’s goal of expanding coverage conflicts with federal priorities.
Medi-Cal is an essential component of California policymakers’ ongoing efforts to achieve universal health coverage. However, the federal government is encouraging states to adopt policies that could decrease coverage, such as making Medicaid subject to work requirements. Reduced federal funding also threatens several large Medi-Cal initiatives. One key project is California’s Whole Person Care pilot program, which uses federal funds to provide more-integrated health and social services for high-cost enrollees, with the goal of reducing health care costs and maintaining budget neutrality.
Sources: For studies on the effects of the ACA Medicaid expansion, see Ghosh, Simon, and Sommers, “The Effect of Health Insurance on Prescription Drug Use Among Low-Income Adults” (2018); Hu et al. “The Effect of the Affordable Care Act Medicaid Expansions on Financial Wellbeing” (2018); Miller and Wherry, “Health and Access to Care during the First Two Years of the ACA Medicaid Expansions” (2017); Simon, Soni, and Cawley, “The Impact of Health Insurance on Preventive Care and Health Behaviors” (2017); and Lindrooth et al. “Understanding the Relationship Between Medicaid Expansions and Hospital Closures” (2018).


